Principle of management in primary bone sarcoma
Allograft for bridging the bone defect
Development and advances in tumor prostheses
Figure 1A: modular tumor prostheses; Figure 1B: custom made tumor prostheses.
Complications
A growing tumor prosthesis for correction of leg shortening
There are two types of growing tumor prosthesis.
Conclusion
Bone sarcoma is a malignant bone tumor. It is commonly referred as bone cancer. Primary bone sarcoma usually occurs in adolescents and young adult. It accounts for 5% of all children cancer. The tumour cells grow abnormally and destroy bone. They can metastasize to lung and other body organs via bloodstream. Before 1970 without systemic chemotherapy, limb amputation was performed only for local control of the disease but not the distant metastases. It explained why only 10-20% patients can survive for longer period.
Principle of management in primary bone sarcoma
The goal of the treatment is to save life by completely removing the tumor from your body. This can be achieved by both systemic chemotherapy and surgical excision of the tumor. We can save the limbs only if tumor can be completely cleared. When tumor is too extensive, or important vessels and nerves of the limbs are involved, amputation should be the treatment of choice. Limb saving surgery should not be attempted if tumor clearance is doubtful.
Limb saving surgery consists of three important steps
1.Completely remove the tumor and achieve good resection margin
2.bone defect and joint reconstruction
3.soft tissue reconstruction to restore function
Metal prosthesis has been used for more than 50 years. However, results of some early metal prosthesis were disappointing, leading many surgeons to use cadaveric bones (allograft) or other methods of reconstruction.
Allograft for bridging the bone defect
Allograft has been used to reconstruct the bone defect after tumor excision for many years. It serves as one form of biological reconstruction to bridge the bone defect. The dead bone will slowly incorporate into host bone and it is hoped that the reconstruction will remain long lasting. However, allograft does have its limitations and complications. The early complications include infection, acute rejection, nonunion and joint instability. The late complications include allograft fracture and bone instability as allograft becomes weak and brittle during the process of bone incorporation. The infection rate can be up to 30%. Uncontrollable infection can result in amputation. Functional outcome can be reasonably good in the first few years but it will deteriorate slowly throughout years.
Development and advances in tumor prostheses
With advances in technology, better prosthetic designs and modern manufacturing techniques, the performance and survival of prosthesis has improved dramatically. We have been using tumor prostheses in Hong Kong since 2003. Our early results are very encouraging and are superior to that of allograft reconstruction.
Tumor prosthesis is a metal implant that is designed to replace a diseased bone or joints, such as hip and knee joints. Common sites for replacement are distal femur, proximal tibia, proximal femur and proximal humerus. Tumor prosthesis is available in modular system. The modular components with different sizes are manufactured before surgery and tumor surgeons can choose the appropriate combinations for the patient at the time of surgery. Tumor prosthesis can also be custom-made (designed and manufactured specifically for a patient). (Figure 1A and 1B) In recent years, tumor surgeons can precisely remove bone tumor and reconstruct the bone defect under the guidance of computer navigation.
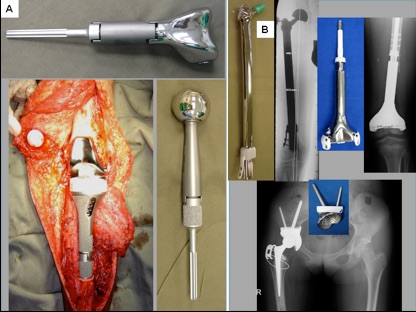
Figure 1A: modular tumor prostheses; Figure 1B: custom made tumor prostheses.
With advancement of modern technology, the metal alloy used for the fabrication of the prosthesis is much stronger, more durable and more inert to our body. The hinge design of the prosthetic joint allows excellent joint motion (flexion, extension and some degrees of rotation) and mimics the normal joint movement. Most of the patients can achieve 80-90% of normal limb function after surgery. This modern design can also help to decrease the stress transmitted to the junctional area of prosthesis with the host bone and thus decrease the chance of loosening. In general, 80-90% of patients with proximal femur tumor prostheses and 70-80% of patients with distal femur tumor prostheses can use their prostheses for more than 10 years.
Complications
There are many factors affecting the outcome of individual tumor prosthesis. Sometimes, it is difficult to predict how long each prosthesis can last.
Specific complications include infection (< 10%), mechanical problems and loosening of the implant.
Just like all artificial implants, metal prosthesis will wear out, break and become loose with time. If patient is young at the time of surgery, the prosthesis will wear out after prolonged use. Revision or replacement might be inevitable.
A growing tumor prosthesis for correction of leg shortening
Bone sarcoma usually grows near the growth plate in children. The growth plate will be removed together with the tumor when surgeons performed the operation. Therefore, the remaining bone will not grow in the operated legs and will lead to leg shortening when the child grows. A special type of custom made growing tumor prosthesis can be used in this situation. When the patient grows, prosthesis can be extended to balance leg length.
There are two types of growing tumor prosthesis.
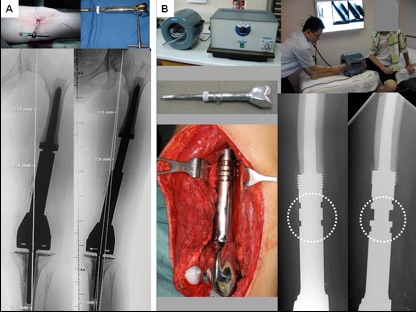
The first one is minimally invasive growing prosthesis. (Figure 2A)
The lengthening procedure is performed in operating theatre. A small incision (1 to 2cm) is made. A special key is inserted into the prosthesis allows extending the prosthesis. This type of growing prosthesis has been used for more than 15 years. It proves to be successful and reliable.
The second type of growing prosthesis is noninvasive growing prosthesis. (Figure 2B)
This has been done successfully for 8 years. Once the patient has the first surgery of putting into the growing prosthesis, subsequent lengthening procedure does not require additional surgery. The growing prosthesis has a powerful magnet mounted inside. Patients only need to put their leg with the prosthesis into a magnet driving machine. The magnet field of the machine enable turning of the magnet and gear drive inside the prosthesis and the prosthesis can be lengthened automatically. The whole procedure can be performed at outpatient clinic. Patients experience no pain and discomfort, can walk immediately and no need to stay in the hospital
Conclusion
Tumor prosthesis is a good option to reconstruct bone defect after surgery on bone tumor. The results of tumor prostheses are more predictable. and successful. Although we may still encounter problems in the long run, as compared with other surgical methods, the results are very promising. The tumor prosthesis will certainly has increasing role in limb saving surgery in coming years.
Dr. WONG, Kwok-chuen