Introduction
Anatomy
Traumas in the shoulder
Cause
Symptoms
Diagnosis
Treatment options
Rehabilitation
Prevention
Introduction
The term shoulder is often referred as the shoulder joint (glenohumeral joint), which is a synovial joint between the head of the humerus and the glenoid fossa of the scapula. Trauma of the shoulder is not uncommon and can happen to anyone of any age.
Anatomy
The shoulder girdle includes three bones, the arm bone (humerus), the slightly S-shaped collarbone (clavicle) and the triangular shoulder blades (scapula). With the corresponding shoulder girdle muscles, tendons, joint capsules and ligaments, these three bones articulate onto the upper thorax. This allows circular and a wide range of other motions of the arm.
The rotator cuff muscles consist of four muscles -- the supraspinatus, subscapularis, infraspinatus and teres minor muscles. They keep the humeral head against the glenoid fossa during different planes of motion. The deltoid muscle is the largest shoulder girdle muscle that envelops the proximal humerus.
The range of motion of the shoulder joint includes flexion, extension, abduction, adduction, internal rotation and external rotation. Proper shoulder function requires co-ordinated motion at three joints (sternoclavicular, acromioclavicular and glenohumeral joints) and one articulation (scapulothoracic articulation). Small, linear movements that take place between the humeral head and glenoid fossa are called translation. When translation is excessive and becomes symptomatic, there is clinical instability.
Traumas in the shoulder
There are different types of shoulder injuries, broadly grouped into two main categories:
1. Bony fractures:
These injuries include fractures of the humerus, the clavicle and the scapula. Combinations of fractures can occur. Fractures involving the nearby rib cage are quite common among patients who have sustained high-impact traumas.
2. Soft tissue injuries:
Common soft tissue injuries include joint dislocations or tendon injuries around the shoulder girdle. Dislocations can involve any of the following three joints: the sternoclavicular, the acromioclavicular or the glenohumeral joints. Dislocations of the glenohumeral joint can become recurrent, causing significant disability, especially among young athletes.
Rotator cuff problem is the commonest tendon injury around the shoulder girdle. Most of the patients who suffer from rotator cuff tears are over the age of 40. It is less common to find this injury among younger people but when they do sustain a tear, it often follows an acute trauma or repetitive overhead work or sports activity.
Cause
There are a wide variety of traumas that can cause the above-mentioned injuries. A clearly defined incident, such as a fall, could cause fractures of the collarbone. Some soft tissue injuries, such as rotator cuff tears, are caused by ill-defined incidents. These injuries are a result of a combination of factors including degeneration, micro-trauma and overuse. For traumas associated with specific accidents, the level of severity differs. Some occur as a result of relatively low impact, such as a trivial fall injury that could cause proximal humerus fracture in an elderly patient with osteoporosis. On the other hand, high-energy traumas, such as high-speed car accidents, can cause multiple major injuries.
Symptoms
Most patients with acute fractures experience severe pain upon any attempt to raise the arm. Other signs suggesting severe injuries include:
bruise and swelling, with or without skin abrasions;
deformity;
severe pain upon any attempt to move the arm; and
weakness or paralysis upon any attempt to move the arm.
If you experience any of the above symptoms, please consult your doctor for a proper assessment.
Diagnosis
Most of the fractures and dislocations around the shoulder girdle can be properly assessed and diagnosed after taking appropriate X-rays. Some injuries such as fractures that are not so obvious may require other imaging studies like CT scan. Examples of these injuries include fracture of the glenoid rim associated with an anterior traumatic dislocation of the shoulder joint. CT scans also allow for better assessments of the displacement of certain bony fragments. MRI (with or without an arthrogram) or Ultrasonogram (USG), are also helpful in assessing soft tissue damages in shoulder injuries, such as rotator cuff tears.
Upon proper history taking, a detailed physical examination and supplementary imaging studies, your orthopaedic surgeon can arrive at the correct diagnosis of the type and severity of your injuries.
Treatment options
Clavicle Fractures
- Most clavicle fractures can be treated conservatively without surgery, either with a brace in the shape of the figure 8 or an arm sling.
Proximal Humerus Fractures
- Most fractures of the proximal humerus in the elderly population have minimal displacement and can be treated conservatively without surgery. If the fragments are displaced significantly, surgery is required. Surgery usually involves reduction of the displaced fragments and fixation of the reduced fragments with metallic plates, screws, pins, sutures or wires. Occasionally, the damage is so severe that it requires shoulder replacement with metallic prosthesis (arthroplasty).
Scapular Fractures
- Most fractures of the scapula can be treated conservatively without surgery. Conservative treatment includes wearing a sling or shoulder immobiliser, which immobilses the shoulder to a much greater extent than a sling. Rest and pain killers can help control pain at the initial stage of rehabilitation. Physical therapy is required to improve the range of motion and to strengthen the muscles of the shoulder girdle. Fractures involving the glenoid fossa or with an additional fracture of the clavicle may need surgical intervention.
Acromioclavicular Joint Separation
- Important factors have to be considered in deciding the appropriate treatment methods for patients with acromioclavicular joint separations. These include severity and direction of the separation, and the physical conditions of the patient. Mild-grade separations can be treated conservatively without surgery. However, higher-grade separations in the upward direction or in the posterior or downward directions of the collarbone often require surgery. Professional athletes and manual laborers are often treated with surgery. However, the results are often unpredictable.
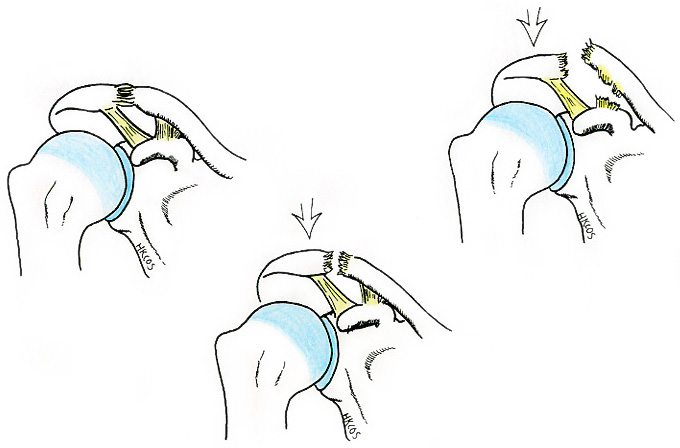
Shoulder Dislocations
- Your orthopaedic surgeon will reduce the ball of the humerus (humeral head) back into the joint socket (glenoid fossa). This process is called closed reduction. Severe pain stops almost immediately once the shoulder joint is reduced. In cases of chronic dislocation, closed reduction may not be possible and may require surgery with open reduction. Once a closed reduction is performed, your orthopaedic surgeon will confirm its success with an X-ray and then immobilise your shoulder in a sling or other device for several weeks. The sore area can be iced for comfort. Controversy exists concerning the use of immobilisation and its duration. This should be discussed with your orthopaedic surgeon.
A shoulder dislocation may be complicated by other associated injuries. For example, associated rotator cuff lesions can cause pain and stiffness in patients of about 40 years old. In these cases, rotator cuff tears may be present and surgical repair may be necessary.
Young people with torn or stretched capsulolabral ligamentous complex can develop recurrent shoulder instability with episodic dislocations. Surgery may be required to repair or tighten the torn or stretched ligaments that help to keep the joint in place.
Rehabilitation
Rehabilitation is an important part of the whole treatment process. Usually, the physical therapy programme begins with gentle and passive motion and, at the appropriate time, advances to active and resistive exercises. The programme will be individualised by your orthopaedic surgeon, physiotherapist and occupational therapist based on your conditions. Complete recovery usually takes several months. A strong commitment to rehabilitation is essential in achieving a good surgical outcome. Your orthopaedic surgeon will assess the final outcome to determine when it is safe for you to return to work and sports activity.
From time to time, there are possible complications associated with shoulder injuries that may need a longer period of rehabilitation or even additional surgical procedures.
Prevention
Since this is a traumatic injury, no prevention measures are available.
俞江山醫生 Dr. YU, Kong-san