Introduction
Steps in CAOS in bone tumour
Pre-operative planning
Resection Plane designed on the virtual bone model. Yellow: bone tumour. Green: tumour with margin
Bone cutting under the computer guidance
Introduction
21St Century is the era of accuracy and precision. With the advancement in computer technology, our accuracy and precision in surgical technique has a great leap forward. One area of the recent development in the computer assisted Orthopaedic Surgery is in the management of bone tumour surgery.
Limb sparing surgery has replaced limb amputation in most situation of bone tumour surgery. By introduction of computer assistance, the amount- to- resected will be as exact as the pre-operative planning. On one hand, we can preserve healthy tissue to allow maximize the overall function of the diseased limb. On the other hand, we can ensure the complete removal of diseased tissue.
Steps in CAOS in bone tumour
This technology was first developed in Hong Kong. It consisted of four crucial steps.
1. pre-operative planning
2. data transfer to intra-operative computer
3. recognition of spatial relationship of bone by computer
4. execution of surgical procedure such as bone cutting under real time computer guidance
Pre-operative planning
Tumour pathology is better shown by the magnetic resonance imaging. The bony structure which is recognized by the intra-operative computer is better visualized by the CT scan. Therefore the first step is to have MRI and CT scan image fusion. It is all by the software work. After fusion, the diseased tissue is marked on the virtual 3-D bone model. The surgical procedures such as bone cut, screws insertion can be planned accordingly on the virtual bone model.
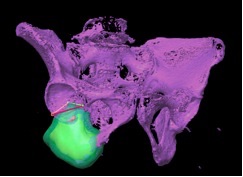
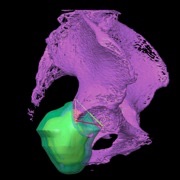
Resection Plane designed on the virtual bone model. Yellow: bone tumour. Green: tumour with margin
Data transfer to the intra-operative computer
The pre-planned surgical planning is then transferred to the intra-operative computer as usual data transfer.
Recognition of spatial relationship of bone by computer
The spatial relationship of patient’s bone has to be recognized by the computer. With the use of navigated instruments and intra-operative X-Ray imaging, the spatial relationship of the patient’s bone can be picked up by the computer.
Execution of surgical procedure
The final step is to execute the pre-planned procedure. Because of the real time computer guidance, bone cut or implant placement will be as exact as planned. It avoids cutting too much or too little in case of tumour resection. Our experience tells us that the error may be less than 1mm on average.

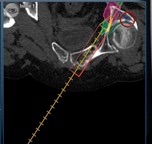
Bone cutting under the computer guidance
Conclusion
The computer assisted bone tumour surgery improves overall accuracy and precision in suitable cases of tumour ablation surgery.
Dr. LAM, Ying-lee