Introduction
Anatomy
Cause
Symptoms
Diagnosis
Non-surgical treatment
Surgical treatment
Rehabilitation
Prevention
Introduction
The term “tennis elbow” is widely used because it was first found among tennis players. However, tennis elbow occurs more frequently among non-athletes than athletes, such as housewives, whose work often involves bending the wrists. Less than 10% of patients having tennis elbow are tennis players. 50% of tennis players experience lateral elbow pain in their lifetimes. There is higher incidence in tennis playing beginners as a result of poor technique.
Anatomy
The tendons involved are responsible for anchoring the muscles that extend or lift the wrist and hand.
Cause
A person would experience pain and pressure in the forearm and hand when in contraction, as in gripping or lifting heavy objects or wringing a towel when they are suffering from tennis elbow. That is because the muscles and fascia for lifting the wrist and fingers have repeated microtears and later become degenerated and painful due to the overuse of these muscles and tendons. There is evidence of acute or chronic inflammatory changes. Besides these, there are no other symptoms.
Symptoms
Less than 5% adults of general population have tennis elbow. It is most prevalent in the fifth decade of life. It equally affects both sexes and is more commonly present in the dominant arm. The risk factors include manually intensive occupations and using vibratory tools.
Patients will have insidious onset of pain after recent changes in occupational or sporting activities. They will have unique discomfort with shaking hands, shaving, lifting luggage or groceries with an extended elbow or raising a coffee mug. In fact, anybody who frequently uses the wrists rigorously is at risk of suffering from tennis elbow. The pain originates in the fascia of the wrist tendons. There is no relationship between tennis elbow pain and pain resulting from a degenerative joint.
Diagnosis
After history taking and physical examination, your doctor will check if you have any pain or discomfort at the bony prominence on the outside of your elbow, as well as pain in the elbow and forearm upon stretching of the wrist and fingers.
Resisted wrist extensor triggers lateral elbow pain when the elbow is in extended position (Cozen’s test). Examination on a flexed elbow will reproduce pain if the degenerative process is more severe. The range of motion of wrist and elbow is full. However, the grip strength will be diminished secondary to the effect of pain. “Chair test” can elicits lateral elbow pain on lifting a chair with a pronated hand.

Cozen's test

Chair test
Lidocaine injection test can also be done. Injection of lidocaine at the origin of extensor carpi radialis brevis tendon can relieve the lateral elbow pain in tennis elbow.
X-ray is usually not necessary for making the diagnosis. It may show mild soft tissue calcifications. However, it can be used to exclude other causes of elbow pain e.g. fractures and osteoarthritis etc. Ultrasound may also show calcification of the common extensor tendon and some focal hypoechoic regions within the tendon, complete or partial discrete cleavage tears and diffuse heterogeneity. Magnetic resonance imaging is usually unnecessary. It is useful for identifying concomitant intra-articular pathology.
Non-surgical treatment
Tennis elbow is self-limiting in vast majority of cases with clearing within 1 year. Non-surgical treatments include physiotherapy e.g stretching exercises, ultrasound treatment, shockwave therapy, non-steroidal anti-inflammatory drugs, orthotics such as elbow braces or splints to relieve tension on the muscle.

(Shockwave therapy)
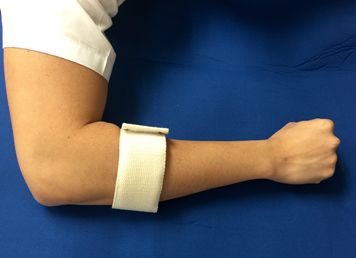
(Elbow band)
Improvement can be seen in around 90% of cases. Doctor will ask you to refrain from repetitive/overuse activities that will aggravate your symptoms. The recurrence rate is less than 5%.
If symptoms do not improve, the next step is a corticosteroid injection around the outside of the elbow. But avoid repeated injections (more than two or three in a specific site).

(Corticosteroid injection)
Surgical treatment
Surgery is rarely needed and is recommended only to patients who have incapacitating pain that does not get better after non-surgical treatment. Around 5-10% of patients will have persistent symptoms after half to one year of non-surgical therapy. The surgery is performed through an incision on the outside of the elbow with excision of the diseased or degenerated tendon fibres, with or without reattachment of the normal tendon fibres to the bone depending on the operative findings under either regional or general anaesthesia. The success rate is more than 90% with good to excellent outcomes.
Rehabilitation
After the surgery, an elbow splint is applied for one to two weeks as recommended by your doctor. This will be followed by gradual stretching exercises. More strenuous activity can be resumed within the limit of pain in 8 to 12 weeks’ time depending on your recovery speed.
Prevention
Regular stretching exercises of the wrist and fingers along with a refrain from overusing the muscles that extend or lift the wrist and hand will help prevent tennis elbow. You may also need to modify or correct your activity at work or in sports to prevent further injury to the muscle fibres.
The Hong Kong Society for Surgery of the Hand