Introduction
Labral tear
Femoroacetabular impingement (FAI)
Loose body
Infection
Synovectomy or biopsy
Snapping hip
Contraindications
Potential complications
Recovery
Future
Introduction
Hip arthroscopy (Fig.1) is one of the fastest-growing areas in orthopaedic surgery. There are many reasons for this, including a better understanding of the pathophysiology of hip joint pathology, improvements in imaging quality and technology advancements in arthroscopic instrumentation. A detailed history taking and physical examination together with the help of imaging studies including X-ray, CT scan, MRI and MR arthrogram are very important in confirming various hip pathologies.
Initially, hip arthroscopy was an instrument primarily for the diagnosis of intra-articular hip pathology. Now, various techniques are being developed to help perform procedures in and around the hip joint that were previously performed by conventional open methods. It has become a surgical modality capable of delivering great therapeutic results.
Hip joint is tight with limited potential space. Therefore hip distraction (Fig.2, Fig.3) is important to allow insertion of arthroscope and instrument in hip joint. A well padded perineal post (Fig.4) which provide counter-traction is important to protect the nerves around the perineum. It is commonly performed under general anaesthesia.

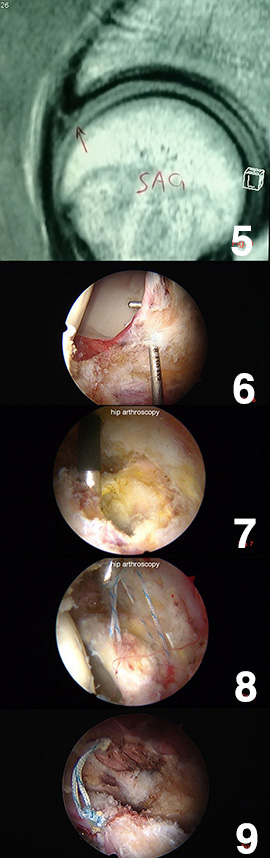
Labral tear
A hip labral tear (Fig.5) involves the ring of cartilage (labrum) that follows the outside rim of the socket of the hip joint. In addition to cushioning, the labrum acts like a rubber seal to help hold the ball at the top of your thighbone securely within your hip socket.
Athletes who participate in sports such as ice hockey, soccer, football, golf and ballet are at higher risk of developing a hip labral tear. Structural abnormalities of the hip also can lead to a hip labral tear.
Labral lesions represent the most common indication for hip arthroscopy. Favorable results can be expected with repair or debridement of painful labral tear (Fig6, Fig7, Fig8, Fig9).
Femoroacetabular impingement (FAI)
FAI occurs when the ball and socket of the hip joint don't fit together properly. The restricted motion damages cartilage and can cause pain and arthritis in young adults.
In some cases, the ball does not fit properly into the socket, we called it CAM lesion (Fig.10). Sometimes, the edge of the socket covers too much of the ball, we called it PINCER lesion (Fig.11). It can also be caused by a combination of these two problems.
Most people with hip impingement experience pain in the groin area during or after flexing the hip, such as when running, jumping or sitting for a long time. You may also have difficulty flexing your hip beyond a right angle.
FAI is increasingly recognized as a factor causative of many labral and articular lesions. It can often be successfully managed with the arthroscope by removing the excessive bone (Fig.12, Fig.13, Fig.14, Fig.15), sometimes reattachment of the labrum is necessary if the excessive bone is over the socket side. However, this is a technically demanding procedure.

Loose body
Removal of symptomatic loose bodies represents the clearest indication for hip arthroscopy. The diagnosis is often evident; the importance of loose body removal is to avoid hip joint damage and improve the mechanical symptom. Arthroscopy offers a much less invasive alternative (Fig.16) to traditional open technique.

Infection
Septic arthritis is a painful infection in a joint. The infection can come from germs that travel through your bloodstream from another part of your body or occur when a penetrating injury delivers germs directly into the joint. It can quickly and severely damage the cartilage and bone within the joint, so prompt treatment is crucial.
Treatment involves surgical draining of the joint and appropriate antibiotics. Arthroscopy (Fig.17) offers a much less invasive alternative to traditional open technique (Fig.18).

Synovectomy or biopsy
Like other joints, there is a role for arthroscopic synovectomy of the hip. Although a complete synovectomy cannot be performed, a generous subtotal synovectomy can be carried out. It also offers s a less invasive alternative to open biopsy of hip joint lesion (Fig.19).

Snapping hip
Snapping hip is a condition in which you feel a snapping sensation or hear a popping sound in your hip when you walk, get up from a chair, or swing your leg around. It is usually painless and harmless but the sensation can be annoying. The commonest cause is due to tight iliotibial band, other causes include iliopsoas tendon, labral tear and cartilage lesion.
Initial treatment typically involves a period of rest and modification of activities. Physiotherapy can also helps and steroid injection may be useful if an painful bursitis is associated. Surgery is indicated if it does not respond to conservative treatment, arthroscopy (Fig.20) offers a much less invasive alternative to traditional open technique.
Contraindications
Careful patient selection is paramount for achieving good outcomes after hip arthroscopy. Contraindications includes arthrodesed hip and advanced osteonecrosis or arthritis.
Potential complications
Complications from hip arthroscopy are uncommon. Any surgery in the hip joint carries a small risk of injury to the surrounding nerves or blood vessels, or the joint itself. The traction needed for the procedure can stretch nerves and cause numbness, but this is usually temporary. There are also small risks of infection, as well as blood clots forming in the legs (deep vein thrombosis).
Recovery
After surgery, pain-killers are often prescribed for pain control. Crutches may be necessary to aid walking or limit the weight bearing over the operated limb. The duration of crutches needed depends on the type of procedure. In most cases, physical therapy is necessary to achieve the best recovery.
Future
In future, we can expect the development of specialized instruments and the refinement of the techniques of these procedures. Currently, the use of computer-assisted collision software to detect areas of femoral-acetabular impact for resection in FAI is being commercialized and used. The future of hip arthroscopy will centre on joint preservation. With the help of hip arthroscopy, biological solutions for the prevention or treatment of articular cartilage problem, such as growth factors, gene therapy and stem cells, are likely to be developed and aid in the preservation of the hip joint.
Dr. LIE Wai-hung, Chester