Introduction
Anatomy
Cause
Symptoms
Diagnosis
Non-surgical treatment
Surgical treatment
Rehabilitation
Introduction
Congenital idiopathic clubfoot is a complex deformity of the foot that affects 0.39 babies per 1000 live births in the Chinese population. It is over twice more common in boys than in girls. Half of babies born with clubfoot have the condition affecting both feet.
Anatomy
Outwardly, the foot appears to be turned inwards. There is tightness of the heel cord (Achilles tendon) which causes the heel to appear very high with a deep skin crease over the heel. There is subluxation of the talo-navicular joint and contracture of the surrounding ligaments and tendons.
.jpg)
Cause
The exact cause of Congenital Idiopathic Clubfoot is still unknown. However, there is often a strong family history: if a first-degree relative e.g. father or mother had clubfoot, then the infant’s chance of having clubfoot is 17 times that of the normal population. The condition has also been linked to maternal smoking during the first trimester of pregnancy.
There is a different type of clubfoot that develops in children with neurological or syndromal disorders like cerebral palsy, spinal dysraphism, and arthrogryposis. The type of clubfoot found in these children is treated differently and have a very different outcome from that of the idiopathic type of clubfoot.
Symptoms
The outward appearance is described in the “Anatomy Section”. It does not cause the infant any pain or distress.
Diagnosis
The condition can be identified prenatally with ultrasound examinations. It is often detected in the routine Anomaly Scan at 18 to 21 weeks of gestation. If it is not detected during the ultrasound, it will be readily apparent at birth. The diagnosis of Congenital Idiopathic Clubfoot will be made in a newborn with the aforementioned foot deformity and in the absence of any neurological or syndromal conditions as discussed above in the “Cause Section”. Xrays are not necessary for diagnosis or initial management of the clubfoot.
Children born with clubfoot will be routinely screened for other “packaging disorders” at birth: developmental dysplasia of the hip and torticollis.
Non-surgical treatment
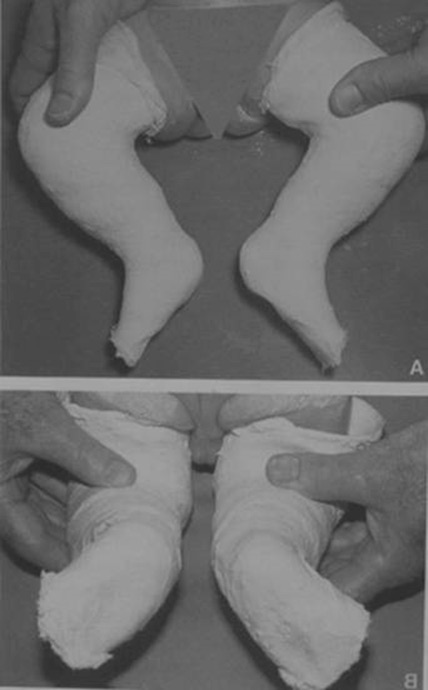
Clubfoot is treated soon after birth by serial casting. The most practised treatment is the Ponseti Technique of serial casting which has excellent long-term outcomes. This technique involves six to eight weeks of long leg plaster casts (from toe to groin). The casts are changed once per week to allow gentle manipulation for deformity correction before the next cast is reapplied. Up to 90% of cases require an Achilles tenotomy to correct the remaining ankle equinus (heel cord tightness) deformity. This is a minor surgical procedure which can be performed with a local anaesthetic and is considered a routine part of the clubfoot treatment after initial Ponseti serial casting. All patients are required to wear a boots- and-bar brace for 23 hours per day for three months and then during sleep until four years of age.
.jpg)

Surgical treatment
Up to 50% of children, after initial Ponseti casting and subsequent boots-and-bars bracing, have residual dynamic deformity of the foot where the tibialis anterior muscle pulls the foot inwards as the child walks. This is addressed by performing tendon transfer surgery to rebalance the musculature around the foot. In severe relapses of the clubfoot deformity, a combination of soft tissue and bony surgery may be necessary.
Rehabilitation
After the infant has completed the serial casting and Achilles tenotomy, the family is usually referred to physiotherapy to continue manual stretching of the heel cord. The infant’s carers will be taught the technique of performing Achilles stretches and will be expected to continue these stretches for the child until the boots-and-bars braces can be discontinued. As the child grows and uses the boots-and-bars brace in his sleep, his daytime activities will not be affected and is expected to have normal gross motor development.
The entire lower limb of the foot affected with clubfoot deformity will be congenitally smaller: there will be a smaller calf muscle bulk and the foot will be smaller than the contralateral side by 1 shoe size. This is due to the congenital abnormality of the entire lower limb and is not a result of the serial casting in infancy. The muscle bulk of the limb will not improve with additional exercises. However, the small muscle bulk and small foot are cosmetic problems only. These children have normal function when compared to their peers.
Dr. Evelyn KUONG