Introduction
Anatomy
Cause
Symptoms
Diagnosis
Non-surgical treatment
Surgical treatment
Rehabilitation
Prevention
Introduction
Impingement of the shoulder is common among young athletes and middle-aged people. Young athletes who use their arms overhead for swimming, baseball and tennis are particularly vulnerable. Those who do repetitive lifting or overhead activities using the arm, such as paper hanging, construction or painting, are also
Anatomy
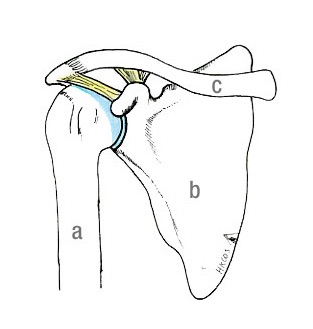
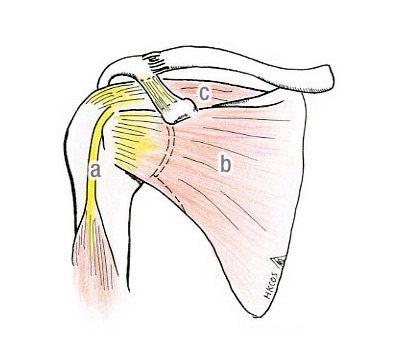
The rotator cuff tendons consist of tendons of four muscles that immediately wrap around the most proximal part of the humerus. They are attached to the greater tuberosity (lateral part) or lesser tuberosity (anterior part) of the proximal humerus. These muscles work together to lift and rotate the shoulder. The acromion is the most cranial part of the shoulder blade (scapula). Together with the coracoacromial ligament (CAL), they cover the superior part of the humeral head.
Cause
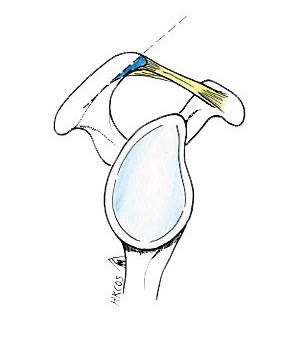
Impingement develops when the tendon at the rotator cuff joint becomes pinched between the greater tuberosity and undersurface of the acromion, and becomes inflamed (tendinosis). The surrounding subacromial bursa (a sac of fluid under the highest part of the shoulder) may also become inflamed (bursitis). These are possible causes of shoulder pain.
Reactive changes may develop on the acromion, with the loss of areolar tissue under the acromion and CAL, the development of thickened fibrous pad, the fibrillation of CAL, and the formation of acromial spur. As the arm is lifted, the acromion and the CAL may exert pressure, or “impinges”, on the rotator cuff tendons. This may cause pain during, or even limit, certain movements of the shoulder.
The pain may be due to soreness of the inflamed rotator cuff tendon (tendinosis). Another common cause of pain is soreness (bursitis) of the subacromial bursa (a sac of fluid under the highest part of the shoulder). In some circumstances, there is a partial tear of the rotator cuff.
Symptoms
You might experience soreness after activities such as painting, lifting or playing a sport that requires lifting the arms. Or you may not remember any specific injury.
Typical symptoms may include:
shoulder pain upon abduction (sideway movement of the arm away from the body);
shoulder pain associated with overhead activities;
pain localised at the anterolateral aspect of the shoulder, which may radiate to the side of the arm;
shoulder pain upon throwing or serving a tennis ball.
In the initial stage, symptoms are usually mild and limited, and most patients do not seek any medical advice at this stage. Pain can often be relieved by over-the-counter pain killers or rest. Gradually, the symptoms may become increasingly disturbing, with more severe pain coming back more often and lasting longer, despite of having rest and treatment.
Diagnosis
Impingement of the shoulder can be diagnosed by proper history taking and a detailed physical examination of the shoulder joint. Plain X-rays and other specific imaging studies, including MRI (with or without an arthrogram) or ultrasound, are also helpful.
The orthopaedic surgeon will perform a detailed examination of the shoulder to see if there is any wasting of rotator muscles. He or she will feel for any particular tender spots and measure the active and passive range of motion of the shoulder joint in different planes of motion to see if there are any impingement signs. He or she will also check for any weakness of the arm and will look for any shoulder instability or other shoulder problems. Depending on the clinical conditions, the orthopaedic surgeon may examine the neck as well, because “shoulder pain” may actually be a result of referred pain from the cervical spine.
Usually, plain X-rays of a shoulder joint show nothing wrong or only minor changes, such as a small subacromial spur or sclerosis of the greater tuberosity. For this reason, the surgeon may need an additional imaging study, either an ultrasound or MRI, for better assessment and documentation of the soft tissue structures deep inside the subacromial space. MRI can sometimes show changes suggesting of tendinosis of the cuff tendons. It can show fluid or inflammation in the subacromial bursa. It can also assess the size, shape and location of the rotator cuff tear. The condition of the biceps tendon can also be assessed.
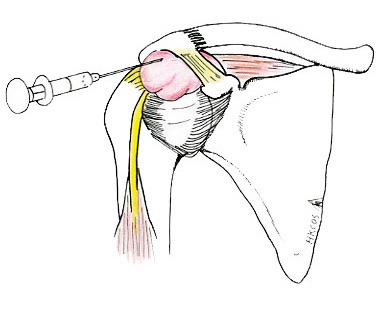
A test that involves injecting a local anesthetic into the subacromial bursa can help to confirm the diagnosis clinically.
Non-surgical treatment
Non-surgical treatment can provide pain relief and improve the function of the shoulder. Options include:
rest and modifications of daily activities;
use of an arm sling;
medications for pain control;
physiotherapy, including rotator cuff-strengthening exercises;
injection of a local anesthetic and a steroid preparation into the subacromial space.
Treatment usually takes several weeks to a few months. Most patients experience a gradual improvement and are able to return to their normal daily activities.
Surgical treatment
Your orthopaedic surgeon may recommend surgery if symptoms persist despite an adequate period of conservative treatment.
During surgery, your orthopaedic surgeon may remove the anteroinferior part of the acromion to tackle the issue of “outlet impingement”. This is because a prominent acromion is thought to cause "impingement" on the cuff tendons and contribute to the pathophysiological changes. The surgery allows the humeral head to move freely in the subacromial space and to lift the arm without pain. Other conditions, including acromioclavicular joint (ACJ) arthritis, the tearing of the biceps tendon or partial rotator cuff tear, may also be addressed by this surgery.
The surgery can take the form of either arthroscopy or open technique.
Arthroscopic technique:
- A fiberoptic scope and appropriate “pen-like” arthroscopic instruments are inserted through several small incisions. This allows the orthopaedic surgeon to perform appropriate surgical repairs under video control. Special instruments are used to remove bone and soft tissue.
Open technique:
- Open surgery requires a small incision. This allows direct visualisation of the acromial spur and acromioplasty performed. Rotator cuff tendons can be assessed accordingly during the surgery.

Rehabilitation
Rehabilitation constitutes an essential part of the whole treatment process. After the surgery, the arm may be placed in a sling for a short period of time, mainly for comfort. A supervised exercise programme will help regain motion and strength. Usually, the physical therapy programme begins with gentle and passive motions and, at the appropriate time, advances to active and resistive exercises.
The programme will be individualised by your orthopaedic surgeon, physiotherapist and occupational therapist based on your conditions. Complete recovery usually takes several months. A strong commitment to rehabilitation is essential to achieving a good surgical outcome. Your orthopaedic surgeon will assess the final outcome to provide advice on when it is safe to return to overhead work and sports activity.
Prevention
One should seek early medical attention if shoulder pain develops because of overuse.
Dr. YU, Kong-san