Introduction
Anatomy
Cause
Symptoms
Diagnosis
Non-surgical treatment
Surgical treatment
Rehabilitation
Prevention
Introduction
Golfer’s elbow is less common than tennis elbow but not limited to golfers. It is sometimes also known as pitcher’s / thrower’s elbow, climber’s elbow or little league elbow. It is actually an overuse injury. Tennis players and others who repeatedly use wrists or clench their fingers also can develop golfer’s elbow.
Anatomy
The tendons involved are responsible for anchoring the muscles that flex the wrist and hand.
Cause
The causes of golfer’s elbow include repeated wrist flexion, particularly against resistance such as holding a golf club. It can also occur from throwing actions, as well as in occupations such as through manual jobs like carpentry or working at a computer work station. It tends to occur after a period of repeated overuse causing microtears between pronator teres and flexor carpi radialis. It is often associated with ulnar neuritis.
Symptoms
Patients will have gradual onset of pain on medial aspect of elbow spreading down into the forearm and wrist. There will be pain when gripping hard with the hand.
Diagnosis
After history taking and physical examination, your doctor will check if you have any pain or discomfort at the bony prominence on the inside of your elbow, as well as pain in the elbow and forearm upon stretching of the wrist and fingers.
Physical examination will elicit tenderness over the flexor origin just anterior and distal to medial humeral epicondyle. The range of motion of wrist and elbow is full. The grip strength will be impaired due to pain. The pain will be reproduced by resisted wrist flexion and pronation.
X-ray is usually not necessary for making the diagnosis. It may show mild soft tissue calcifications at the common flexor origin. However, it can be used to exclude other causes of elbow pain e.g. fractures and osteoarthritis etc.
Non-surgical treatment
The non-surgical treatments for golfer’s elbow include rest, physiotherapy (e.g. stretching exercises, ultrasound treatment, shockwave therapy), orthotics such as elbow braces or splints to relieve tension on the muscles and non-steroidal anti-inflammatory drug.
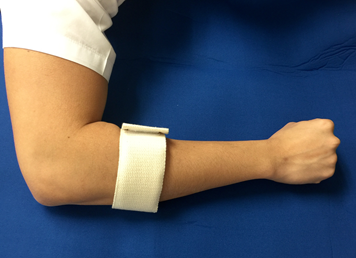
(Elbow band)
Improvement can be seen in around 90% of cases. Doctor will ask you to refrain from repetitive/overuse activities that will aggravate your symptoms.
If symptoms do not improve, the next step is a corticosteroid injection around the inside of the elbow. But avoid repeated injections (more than two or three in a specific site).

(Corticosteroid injection)
Surgical treatment
Less than 10% of patients need surgical treatment which is debridement and release of the flexor pronator origin or reattachment of muscle origin. Most patients often only require partial debridement of flexor carpi radialis and pronator teres origin. Anterior transposition of ulnar nerve is also necessary in case of ulnar neuritis.
Rehabilitation
After the surgery, an elbow splint is applied for one to two weeks as recommended by your doctor. This will be followed by gradual stretching exercises. More strenuous activity can be resumed within the limit of pain in 8 to 12 weeks’ time depending on your recovery speed.
Prevention
Regular stretching exercises of the wrist and fingers along with a refrain from overusing the muscles that flex the wrist and hand will help prevent golfer’s elbow. You may also need to modify or correct your activity at work or in sports to prevent further injury to the muscle fibres.
The Hong Kong Society for Surgery of the Hand