Introduction
Anatomy
Cause
Symptoms
Diagnosis
Non-surgical treatment
Surgical treatment
Rehabilitation
Prevention
Introduction
Numbness and weakness of the hand is a common condition in the adult population. Entrapment of the ulnar nerve is one of the causes of this condition. When the ulnar nerve is “entrapped” at the elbow level, it causes numbness, weakness and even deformity of the ring and little fingers. This is called cubital tunnel syndrome.
Anatomy
The cubital tunnel is a tunnel of tissue behind the inside of the elbow, which travels under muscles on the inside of the arm and into the hand on the side of the palm with the little finger.
Cause
Cubital tunnel syndrome is caused by the compression of the ulnar nerve, which can be due to the inflammation of fascia, muscle degeneration or bone spur at the elbow joint.
Those who have fractured or overused their elbow joints and those who have difficulty straightening the joint are more prone to getting this syndrome.
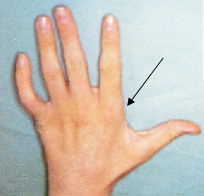
Symptoms
An early sign of the cubital tunnel syndrome is numbness in the little finger and the half of the ring finger that is near the little finger. At a later stage, the hypothenar muscles right below the little finger on the palm side would appear to have signs of degeneration. Even worse, the little and ring fingers become weak and show “clawing”, an apparent deformity when opening up the palm.
Diagnosis
To diagnose the syndrome, an orthopaedic specialist will ask about the typical symptoms and possible predisposing risk factors causing cubital tunnel syndrome. A physical examination including flexion test, tinel sign, and neurological examination of the hand will be performed. Any muscle wasting, reduced sensation of the ring finger, little finger and dorsum of the hand as well as the overall function of the fingers will be tested. In severe cases, a deformity known as the clawed hand will be obvious. Examination of the elbow joint may show prominent bony spur and reduced range of motion suggesting the cause of the nerve compression. A plain X-ray of the elbow will help to confirm the site of ulnar nerve impingement by the bony spur around the elbow. More objective tests – electrophysiological studies including electromyography (EMG) and nerve conduction test (NCV) – can help to confirm the diagnosis.


Non-surgical treatment
During the early stage, the patient can try the following non-surgical methods:
Use an elastic or leather brace to keep the elbow in extension to reduce the pressure on the ulnar nerve
A corticosteroid injection into the cubital tunnel to control the inflammation and swelling
Surgical treatment
Surgery would be recommended if the non-surgical treatment methods are not effective, or if the symptoms are at an advanced stage so that the hypothenar muscles have degenerated, or if a tumor is suspected during a physical examination.
Electrophysiological studies including electromyography and nerve conduction test will be performed before the surgery to confirm if the ulnar nerve is being compressed inside the cubital tunnel.
A cubital tunnel surgery usually involves local or general anesthesia. The patient is allowed to go home within two to three days. During the surgery, the cubital tunnel will be examined and the ulnar nerve will be released and moved from behind to the front of the elbow. Usually, the surgery is an open type that involves the removal of abnormal fascia tissues and the release of the ulnar nerve.
Rehabilitation
After the surgery, the patient will need to wear a cast or splint for two weeks to stabilise the elbow joint. Afterwards, mobilisation and strengthening exercises of the fingers will help the patient restore normal functions.
Prevention
Limit the amount of time performing tasks that require frequent bending of the elbow, such as pulling levers, reaching or lifting. This can prevent irritation of the ulnar nerve. Constant direct pressure on the elbow over time may also lead to cubital tunnel syndrome. The nerve can be irritated from leaning on the elbow while you sit at a desk or from using the elbow rest during a long drive or while running machinery. Take frequent breaks. If necessary, work with your supervisor to modify your job activities.
Dr. NGAI, Wai-kit