Introduction
Anatomy
Cause
Symptoms and Diagnosis
Treatment
Surgical treatment
Introduction
If a child’s feet face inwards or outwards when walking, it is a common physical condition that will disappear naturally as the child reaches around two years of age – or the latest, by eight years. There is no need to make the child wear any corrective shoes or to perform any stretching maneuvers or surgeries on the child. Some parents worry that this condition may develop into a permanent deformity and therefore request doctors to correct the lower leg alignment. However, this worry is unnecessary.

Anatomy
When a child is still in the mother’s womb, the limbs are curled up. At the time of birth, there is a tendency for the hip to rotate inwards, which is why the lower limbs and the feet tend to rotate inwards.
Cause
There are three possible causes accounting for childhood pigeon toes: internal rotation of the femur, internal rotation of the tibia or metatarsus adductus.
On the other hand, duck feet can arise from the external rotation of the femur. Toddlers tend to sleep face down, causing the hip to be rotated outward. This external rotation of the hip usually corrects itself when the children start walking.
Symptoms and Diagnosis
Severe internal tibial torsion may cause the child to stumble and fall, but it normally does not cause any foot pain, neither does it hinder the child from walking. There is not enough evidence linking the internal rotation of femur in childhood to degenerative arthritis in adulthood.
Severe internal femoral rotation would cause the child’s knees to face inwards and to walk with an intoeing gait. This condition is most obvious around the age of 5 or 6 and in most cases, the condition corrects itself before adolescence.
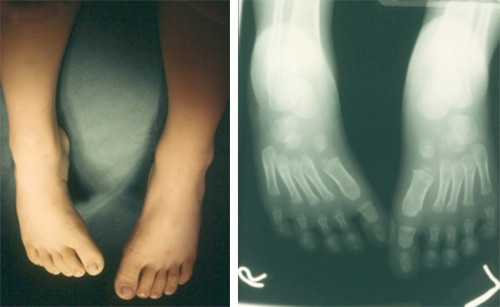
Deviation of metatarsal bones toward the inner side of the foot (metatarsus adduction) may cause intoeing as well. Severe metatarsus adduction may look like club feet, appear like hooves of horse. This condition normally corrects itself as the child grows.
Treatment
For internal tibial torsion, internal femur rotation and external femur rotation, orthotics or other corrective devices are usually unnecessary, because children outgrow the conditions as they grow up.
However, a small percentage of femur rotation cases may be due to rickets or other forms of skeletal dysplasia. An orthopaedic surgeon will be able to advice treatment according to the diagnosis.
Occasionally, children who have genuine metatarsal adductus deformity may require wearing some supportive devices or orthotic shoes to help correct the shape of their feet.
Surgical treatment
If internal tibial torsion or internal femur rotation does not correct itself by the age of 8 to 10, and if the condition hinders the child from walking properly, corrective surgery might be necessary.
Dr. MAK, Kan-hing